Serotonin & Norepinephrine Reuptake Inhibitor's (SNRI's)
Venlafaxine: #1 Prescribed SNRI
Venlafaxine: #1 Prescribed SNRI
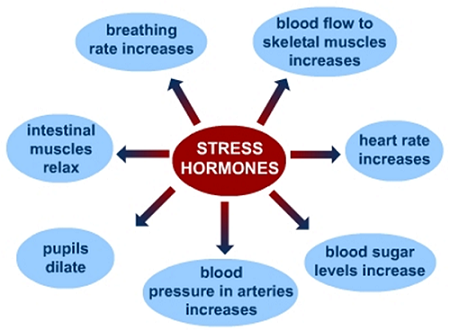 Figure 1. Norepinephrine's sympathetic effects on the body [4]
Figure 1. Norepinephrine's sympathetic effects on the body [4]
Introduction
As described previously GAD is a psychiatric disorder characterized by excessive anxiety and worry about a variety of different things that have been occurring for at least 6 months and that influence multiple aspects of a persons life. This dibilitating disorder can effect sleep and mood, social behavior, and memory. Two major neurotransmitter (chemicals released by neurons, i.e. the cells of the brain) pathways that have been found to be effected by this disorder are the Seratonergic pathway as described previously in the SSRI section and the Noradrenergic (Norepinephrine) pathway. Norepinephrine (also known as noradrenaline) is released from the sympathetic nervous system in response to stress [4]. It signals the start of our "fight versus flight" response, meaning either get ready to fight for your life or run for your life. Norepenephrine is also known as the stress hormone due to its effect on the body (see figure 1). Norepinephrine slows down parasympathetic activities such as digestion and increases sympathetic activities such as increasing heart rate, the amount of glucose being sent to the muscles and the brain, and pupil dilation. It has been shown that SNRI's caused decreased levels of blood pressure, Saccadic Eye Movements (quick eye movements) and cortisol for those treated for GAD [5]. SNRI's are prescribed for depression and anxiety due to low levels of serotonin and norepinephrine in the brain. It is believed that an increase of these neurotransmitters is what alleviates symptoms of GAD [6]. For norepinephrine specifically, an increase in this neurotransmitter would increase levels of alertness and energy, the added alertness can potentially be partially responsible for the alleviation of anxiety symptoms [5]. Forms of SNRI's approved by the FDA include Desvenlafaxine (Pristiq, Khedezla), Duloxetine (Cymbalta), which are approved to treat anxiety and certain types of chronic pain, Levomilnacipran (Fetzima) and Venlafaxine (Effexor XR), which are also approved to treat anxiety and panic disorder [11]. Each SNRI has a slightly different chemical make-up so some may be better suited to individuals than others but all do the same thing, ask your doctor which one is right for you. These can be taken with a combination of other therapies to boost the effects.
As described previously GAD is a psychiatric disorder characterized by excessive anxiety and worry about a variety of different things that have been occurring for at least 6 months and that influence multiple aspects of a persons life. This dibilitating disorder can effect sleep and mood, social behavior, and memory. Two major neurotransmitter (chemicals released by neurons, i.e. the cells of the brain) pathways that have been found to be effected by this disorder are the Seratonergic pathway as described previously in the SSRI section and the Noradrenergic (Norepinephrine) pathway. Norepinephrine (also known as noradrenaline) is released from the sympathetic nervous system in response to stress [4]. It signals the start of our "fight versus flight" response, meaning either get ready to fight for your life or run for your life. Norepenephrine is also known as the stress hormone due to its effect on the body (see figure 1). Norepinephrine slows down parasympathetic activities such as digestion and increases sympathetic activities such as increasing heart rate, the amount of glucose being sent to the muscles and the brain, and pupil dilation. It has been shown that SNRI's caused decreased levels of blood pressure, Saccadic Eye Movements (quick eye movements) and cortisol for those treated for GAD [5]. SNRI's are prescribed for depression and anxiety due to low levels of serotonin and norepinephrine in the brain. It is believed that an increase of these neurotransmitters is what alleviates symptoms of GAD [6]. For norepinephrine specifically, an increase in this neurotransmitter would increase levels of alertness and energy, the added alertness can potentially be partially responsible for the alleviation of anxiety symptoms [5]. Forms of SNRI's approved by the FDA include Desvenlafaxine (Pristiq, Khedezla), Duloxetine (Cymbalta), which are approved to treat anxiety and certain types of chronic pain, Levomilnacipran (Fetzima) and Venlafaxine (Effexor XR), which are also approved to treat anxiety and panic disorder [11]. Each SNRI has a slightly different chemical make-up so some may be better suited to individuals than others but all do the same thing, ask your doctor which one is right for you. These can be taken with a combination of other therapies to boost the effects.
 Figure 2. Company Responsible for Producing Venlafaxine
Figure 2. Company Responsible for Producing Venlafaxine
Brief History of Venlafaxine
Venlafaxine was first synthesized in the 1980's by John Yardley, Morris Husbands, and Eric Muth (researchers at Wyeth Pharmaceuticals) and has been in use to treat depression since 1994. It was later found to have potential benefits for other disorders such as GAD with its extended-release formulation and has been in use for those since around 1997. [1]
Venlafaxine was first synthesized in the 1980's by John Yardley, Morris Husbands, and Eric Muth (researchers at Wyeth Pharmaceuticals) and has been in use to treat depression since 1994. It was later found to have potential benefits for other disorders such as GAD with its extended-release formulation and has been in use for those since around 1997. [1]
 Figure 3. Capsule form of Venlafaxine (Effexor RX)
Figure 3. Capsule form of Venlafaxine (Effexor RX)
Basic Overview
Venlafaxine (Effexor RX) is a generic antidepressant drug that comes in three forms: an oral tablet, an extended-release oral tablet, and an extended-release oral capsule. The capsule is the most highly prescribed form for GAD, the other two are mostly prescribed for depression. It is classified as an SNRI (Seratonin and Norepinephrine Reuotake Inhibitor) meaning that it effects both the seratonin transmitter and the norepinephrine transmitter. This dual approach is most likely why it is recommended so highly as it effects two different neurotransmitter pathways where anxiety may have effects. It's interaction occurs when it is metabolized to O-desmethylvenlafaxine or desvenlafaxine, two metabolites that inhibit the neuronal reuptake of serotonin as well as norepinephrine. By increasing the amount of seratonin and norepinephrine in the brain, the effects of depression and anxiety have been shown to be reduced for some patients. While this is not a "one drug fits all" kind of prescription, it is the second most highly recommended treatment as stated by the New York Times for GAD, but it should not be taken by people under the age of 18.
Venlafaxine (Effexor RX) is a generic antidepressant drug that comes in three forms: an oral tablet, an extended-release oral tablet, and an extended-release oral capsule. The capsule is the most highly prescribed form for GAD, the other two are mostly prescribed for depression. It is classified as an SNRI (Seratonin and Norepinephrine Reuotake Inhibitor) meaning that it effects both the seratonin transmitter and the norepinephrine transmitter. This dual approach is most likely why it is recommended so highly as it effects two different neurotransmitter pathways where anxiety may have effects. It's interaction occurs when it is metabolized to O-desmethylvenlafaxine or desvenlafaxine, two metabolites that inhibit the neuronal reuptake of serotonin as well as norepinephrine. By increasing the amount of seratonin and norepinephrine in the brain, the effects of depression and anxiety have been shown to be reduced for some patients. While this is not a "one drug fits all" kind of prescription, it is the second most highly recommended treatment as stated by the New York Times for GAD, but it should not be taken by people under the age of 18.
Recommended Dosages (Adapted from healthline.com) [2]
Generic: venlafaxine
Form: oral tablet
Strengths: 25 mg, 37.5 mg, 50 mg, 75 mg, 100 mg
Form: extended-release oral tablet
Strengths: 37.5 mg, 75 mg, 150 mg
Form: extended-release oral capsule
Strengths: 37.5 mg, 75 mg, 150 mg
Brand: Effexor XR
Form: extended-release oral capsule
Strengths: 37.5 mg, 75 mg, 150 mg
Adult dosage (ages 18 years and older)
Special considerations:
People with liver problems: People with mild to moderate liver problems should take about half of the typical dose. People with severe liver disease or cirrhosis may need an even lower dosage. Your doctor can tell you more.
People with kidney problems: People with mild to moderate kidney problems should take 75% of the typical dosage. People who are on dialysis should take half of the typical dosage. Your doctor can tell you more.
Essentially, each dosage varies from person to person so consult with your doctor before making any changes to dosage.
You should take Venlafaxine with food and at doctor recommended times. You can cut or crush this drug. For other concerns see [2].
Generic: venlafaxine
Form: oral tablet
Strengths: 25 mg, 37.5 mg, 50 mg, 75 mg, 100 mg
Form: extended-release oral tablet
Strengths: 37.5 mg, 75 mg, 150 mg
Form: extended-release oral capsule
Strengths: 37.5 mg, 75 mg, 150 mg
Brand: Effexor XR
Form: extended-release oral capsule
Strengths: 37.5 mg, 75 mg, 150 mg
Adult dosage (ages 18 years and older)
- Extended-release oral capsules:
- Typical starting dosage:
- 75 mg per day, given in a single dose in the morning or evening.
- Some patients with generalized anxiety should start at a lower dosage of 37.5 mg per day for 4–7 days.
- Dosage increases: For generalized anxiety, your doctor may increase your dosage by 75 mg per day if needed. Increases should be made no more than every 4 days.
- Maximum dosage:
- For generalized anxiety: 225 mg per day
- For social anxiety: 75 mg per day
- Typical starting dosage:
Special considerations:
People with liver problems: People with mild to moderate liver problems should take about half of the typical dose. People with severe liver disease or cirrhosis may need an even lower dosage. Your doctor can tell you more.
People with kidney problems: People with mild to moderate kidney problems should take 75% of the typical dosage. People who are on dialysis should take half of the typical dosage. Your doctor can tell you more.
Essentially, each dosage varies from person to person so consult with your doctor before making any changes to dosage.
You should take Venlafaxine with food and at doctor recommended times. You can cut or crush this drug. For other concerns see [2].
 Figure 4. Metabolism of Venlafaxine into O-desmethylvenlafaxine through CYP2D6 in the liver [3]
Figure 4. Metabolism of Venlafaxine into O-desmethylvenlafaxine through CYP2D6 in the liver [3]
Metabolism, Psychopharmacology, and Neurochemical Effects
Venlafaxine's metabolized products work as direct antagonists (takes the space of normal neurotransmitters on the receptor [i.e. a lock and key model]) to the serotonergic reuptake receptors at a low dose (50 mg per day) and is both a sertonergic reuptake antagonist and a norepinephrine transmitter antagonist when the dose is increased to around 100-225 mg per day. Essentially, at low doses, O-desmethylvenlafaxine works as an SSRI (Selective Serotonergic Reuptake Inhibitor) but at higher doses it works as both an SSRI and a norepinephrine transmitter inhibitor (i.e. SNRI). The other metabolic form of Venlafaxine called Desvenlafaxine works as an SNRI no matter what the dosage (see [3] for video). In fact, Venlafaxine is five times more potent as a SERT (or 5-HTT, the seratonin transmitter) inhibitor than as a NET (norepinephrine transmitter) inhibitor. Depending on the person taking the drug, this could have great benefits or it could be a non-factor (hence why there are so many medications for GAD).
Venlafaxine gets metabolized in the liver by the 2D6 version of cytochrome P450 (CYP2D6) into O-desmethylvenlafaxine, which is the active ingredient in the available drug form. From there it travels through the blood stream and into the brain where it interacts with the transmitters mentioned above. However, Venlafaxine is also a weak inhibitor of the CYP2D6 so if there are other drugs being taken that are poor metabolizers of CYP2D6 such as MAOI's (Monoamine oxidase inhibitors), then the other form of Venlafaxine, Desvenlafaxine may be more suitable for use due to potential side effects (described below). It has been shown that Desvenlafaxine has no significant effect on CYP2D6 so it wouldn't have a drug to drug interaction as Venlafaxine could potentially have. Both of these kinds of Venlafaxine interact in the same way with CYP2D6 (see [3] for video).
Venlafaxine's metabolized products work as direct antagonists (takes the space of normal neurotransmitters on the receptor [i.e. a lock and key model]) to the serotonergic reuptake receptors at a low dose (50 mg per day) and is both a sertonergic reuptake antagonist and a norepinephrine transmitter antagonist when the dose is increased to around 100-225 mg per day. Essentially, at low doses, O-desmethylvenlafaxine works as an SSRI (Selective Serotonergic Reuptake Inhibitor) but at higher doses it works as both an SSRI and a norepinephrine transmitter inhibitor (i.e. SNRI). The other metabolic form of Venlafaxine called Desvenlafaxine works as an SNRI no matter what the dosage (see [3] for video). In fact, Venlafaxine is five times more potent as a SERT (or 5-HTT, the seratonin transmitter) inhibitor than as a NET (norepinephrine transmitter) inhibitor. Depending on the person taking the drug, this could have great benefits or it could be a non-factor (hence why there are so many medications for GAD).
Venlafaxine gets metabolized in the liver by the 2D6 version of cytochrome P450 (CYP2D6) into O-desmethylvenlafaxine, which is the active ingredient in the available drug form. From there it travels through the blood stream and into the brain where it interacts with the transmitters mentioned above. However, Venlafaxine is also a weak inhibitor of the CYP2D6 so if there are other drugs being taken that are poor metabolizers of CYP2D6 such as MAOI's (Monoamine oxidase inhibitors), then the other form of Venlafaxine, Desvenlafaxine may be more suitable for use due to potential side effects (described below). It has been shown that Desvenlafaxine has no significant effect on CYP2D6 so it wouldn't have a drug to drug interaction as Venlafaxine could potentially have. Both of these kinds of Venlafaxine interact in the same way with CYP2D6 (see [3] for video).
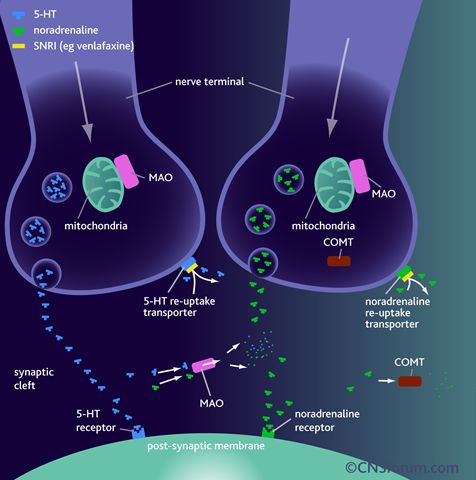 Figure 5. Neurochemical effects of SNRI venlafaxine
Figure 5. Neurochemical effects of SNRI venlafaxine
As stated above, SNRI's block the reuptake of serotonin and norepinephrine by directly binding to their reuptake receptors (see fig 5). 5-HT is another name for serotonin and the nerve terminal is equivalent to the presynaptic terminal button of the neuron. As you can see, the SNRI Venlafaxine is able to block both the serotonergic reuptake receptors and the noradrenergic (norepinephrine) reuptake receptors, effectively leaving larger amounts of both neurotransmitters in the synaptic cleft. With the higher amount being available for the postsynaptic membrane, these neurotransmitters can bind with higer affinity to their postsynaptic receptors where they then are able to regulate the neurochemistry of the brain further. Norepinephrine receptors are found mainly in the muscles of the heart and skeletal muscles and come in two different forms, alpha and beta receptors [7]. The beta1 receptor is seen in the heart where as the beta2 receptor is seen in vascular and non-vascular smooth muscle. Norepoinephrine however only acts on the beta1 receptors. There are also alpha1 and alpha2 receptors that both norepinephrine and epinephrine act on. Norepinephrine when acting on alpha2 receptors, inhibits its release from the presynaptic terminal button [6]. When acting on beta1 receptors, vasoconstriction occurs. These receptors can be either excitatory (beta1 and alpha1) or inhibitory (beta2 and alpha2) which help explain how norepinephrine could potentially aid in the relief of symptoms for GAD.
 Figure 6. Production of norepinephrine in the brain by conversion
Figure 6. Production of norepinephrine in the brain by conversion
Primary Noradrenergic Pathway in the Brain and Noreponephrine Origin
While serotonin is made in the gastrointestinal tract, norepinephrine is released in the adrenal medulla where it and epinephrine are made by adrenal medulla cells that can then effect numerous areas of the body by traveling through the bloodstream [8]. Norepinephrine can also be produced in the postganglionic neurons of the sypathetic nervous system in the same way that the brain can produce its supply. The brain produces its supply of norepinephrine in the locus coeruleus by converting previous catecholemines (a chemical made from the amino acid tyrosine [10]) in the synaptic vessicles from phenylalanine to norepinephrine before neurotransmitter release [9] (see figure 6). Phenylalanine is converted to Tyrosine by phenylalanine hydroxylase which is then converted to DOPA by tyrosine hydroxylase to Dopamine by Aromatic L-amino acid decarboxylase and finally to norepinephrine by dopamine beta-hydroxylase. Norepinephrine can later by converted into epinephrine if needed. The need for the different areas of norepinephrine production is due to its inability to pass the blood brain barrier with high affinity (similar to serotonin).
While serotonin is made in the gastrointestinal tract, norepinephrine is released in the adrenal medulla where it and epinephrine are made by adrenal medulla cells that can then effect numerous areas of the body by traveling through the bloodstream [8]. Norepinephrine can also be produced in the postganglionic neurons of the sypathetic nervous system in the same way that the brain can produce its supply. The brain produces its supply of norepinephrine in the locus coeruleus by converting previous catecholemines (a chemical made from the amino acid tyrosine [10]) in the synaptic vessicles from phenylalanine to norepinephrine before neurotransmitter release [9] (see figure 6). Phenylalanine is converted to Tyrosine by phenylalanine hydroxylase which is then converted to DOPA by tyrosine hydroxylase to Dopamine by Aromatic L-amino acid decarboxylase and finally to norepinephrine by dopamine beta-hydroxylase. Norepinephrine can later by converted into epinephrine if needed. The need for the different areas of norepinephrine production is due to its inability to pass the blood brain barrier with high affinity (similar to serotonin).
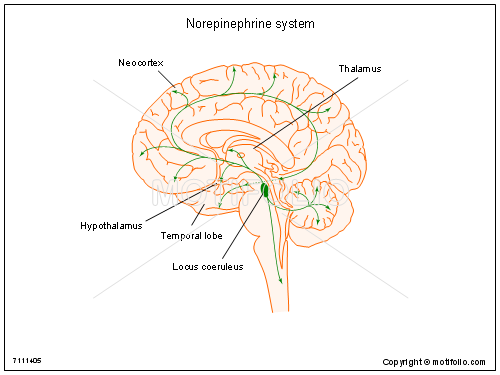 Figure 7. The noradrenergic (norepinephrine) pathway
Figure 7. The noradrenergic (norepinephrine) pathway
The main pathway of norepinephrine in the brain starts at the locus coeruleus (see figure 7). It then projects bilaterally throughout the brain and hits key locations such as the neocortex, the spinal cord, and the limbic system (hippocampus, thalamus and hypothalamus, amygdala, etc.) [10]. Norepinephrine can also be released from the lateral tegmental area where its pathway mainly effects the hypothalamus. These areas of the brain are mainly important for release of hormones (hypothalamus), integration of sensory information and descision processing (thalamus), social behavior and understanding as well as decision processing (neocortex), and some aspects of movement (spinal cord). All in all with the various areas that thes pathways project to, it is quite clear that this neurotransmitter effects many differnt aspects on behavioral and psychological functioning.
Side Effects (some may be due to dosage amounts [12])
Venlafaxine may cause drowsiness. It may also affect your ability to make decisions, think clearly, or react quickly. You should not drive, use heavy machinery, or do things that require you to be alert until you know you can function normally.
Venlafaxine can cause unusual dreams, sexual problems such as decreased interest in sex, impotence (not being able to get or keep an erection), or trouble having an orgasm, loss of appetite, constipation, nausea or vomiting, dry mouth, tiredness, trouble sleeping or change in sleep habits, yawning, tremor or shaking, dizziness, blurry vision, sweating, feling anxious, nervous, or jitterey, headache, and increased heart rate. If these effects are mild, they may go away within a few days or a couple of weeks. If they’re more severe or don’t go away, talk to your doctor or pharmacist.
Other more serious side effects include attempts to commit suicide, acting on dangerous impulses, aggressive or violent behavior, thoughts about suicide or dying, new or worsened depression, new or worsened anxiety or panic attacks, agitation, restlessness, anger, or irritability, trouble sleeping, serotonin syndrome (high body temperature, agitation, increased reflexes, tremor, sweating, dilated pupils, and diarrhea).
If you or a loved one are feeling any of these symptoms call your doctor right away or call 9-1-1 if your symptoms feel life-threatening or if you think you’re having a medical emergency.
Other serious side effects include agitation, hallucinations (seeing or hearing something that isn’t there), coma, changes in your mental status, coordination problems, muscle twitching or overactive reflexes, fast heart rate, high or low blood pressure, diarrhea, muscle stiffness, chest pain, or Mania.
Venlafaxine can also cause greatly increased energy, racing thoughts, reckless behavior, unusually grand ideas, excessive happiness or irritability, talking more or faster than usual, seizures, eye problems such as eye pain, vision changes, enlarged pupils, swelling or redness in or around your eyes, and low sodium levels which can cause weakness, feeling unsteady, confusion, problems concentrating, thinking or memory problems, bruising easily, frequent nosebleeds, frequent bleeding from your gums while brushing your teeth or flossing, dark, tar-like stool, bleeding from wounds that's hard to stop, lung disease or pneumonia. These last two can cause shortness of breath that gets worse, cough, or chest discomfort (See [11] for statistics on side effect occurance rates).
Taking venlafaxine with certain medications raises your risk of side effects. Examples of these drugs include:
Cimetidine
Taking this drug with venlafaxine raises your risk of high blood pressure or liver disease. These risks are greater if you are a senior.
Haloperidol
Taking this drug with venlafaxine raises your risk of QT prolongation. This is a heart condition with symptoms such as dizziness and an irregular heart rhythm.
Warfarin
Taking this drug with venlafaxine raises your risk of bleeding. Your doctor will monitor you closely, especially when starting or stopping your venlafaxine therapy. Tell your doctor right away if you notice any abnormal bleeding or bruising.
Anti-inflammatory drugs such as aspirin, ibuprofen, naproxen, and ketoprofen
Taking any of these drugs with venlafaxine raises your risk of bleeding. Your doctor will monitor you closely, especially when starting or stopping your venlafaxine therapy. Tell your doctor right away if you notice any abnormal bleeding or bruising.
Drugs such as ritonavir, clarithromycin, or ketoconazole
Drugs such as ritonavir, clarithromycin, or ketoconazole can slow the breakdown of drugs in your body. If you take any of these drugs with venlafaxine, the amount of venlafaxine may build up in your body. This would increase your risk of side effects.
Drugs that cause drowsiness, such as zolpidem, lorazepam, and diphenhydramine
Taking any of these drugs with venlafaxine may make the sleepiness from venlafaxine even worse.
Other drugs that can increase serotonin levels, such as fluoxetine, paroxetine, citalopram, duloxetine, linezolid, lithium, tramadol, and methylene blue
Venlafaxine increases your levels of serotonin. Taking it with any of these drugs may increase your serotonin levels even more. If your serotonin levels are too high, a life-threatening condition called serotonin syndrome can occur. Your doctor will monitor you closely when starting or increasing your dosage of either drug.
Certain drugs for migraine, called triptans, such as sumatriptan, rizatriptan, and zolmitriptan
Venlafaxine increases your levels of serotonin. Taking it with any of these drugs may increase your serotonin levels even more. If your serotonin levels are too high, a life-threatening condition called serotonin syndrome can occur. Your doctor will monitor you closely when starting or increasing your dosage of either drug.
Metoprolol
Metoprolol may be less effective when you take it with venlafaxine. This may cause your blood pressure to rise. Talk to your doctor before taking these drugs together.
Venlafaxine may cause drowsiness. It may also affect your ability to make decisions, think clearly, or react quickly. You should not drive, use heavy machinery, or do things that require you to be alert until you know you can function normally.
Venlafaxine can cause unusual dreams, sexual problems such as decreased interest in sex, impotence (not being able to get or keep an erection), or trouble having an orgasm, loss of appetite, constipation, nausea or vomiting, dry mouth, tiredness, trouble sleeping or change in sleep habits, yawning, tremor or shaking, dizziness, blurry vision, sweating, feling anxious, nervous, or jitterey, headache, and increased heart rate. If these effects are mild, they may go away within a few days or a couple of weeks. If they’re more severe or don’t go away, talk to your doctor or pharmacist.
Other more serious side effects include attempts to commit suicide, acting on dangerous impulses, aggressive or violent behavior, thoughts about suicide or dying, new or worsened depression, new or worsened anxiety or panic attacks, agitation, restlessness, anger, or irritability, trouble sleeping, serotonin syndrome (high body temperature, agitation, increased reflexes, tremor, sweating, dilated pupils, and diarrhea).
If you or a loved one are feeling any of these symptoms call your doctor right away or call 9-1-1 if your symptoms feel life-threatening or if you think you’re having a medical emergency.
Other serious side effects include agitation, hallucinations (seeing or hearing something that isn’t there), coma, changes in your mental status, coordination problems, muscle twitching or overactive reflexes, fast heart rate, high or low blood pressure, diarrhea, muscle stiffness, chest pain, or Mania.
Venlafaxine can also cause greatly increased energy, racing thoughts, reckless behavior, unusually grand ideas, excessive happiness or irritability, talking more or faster than usual, seizures, eye problems such as eye pain, vision changes, enlarged pupils, swelling or redness in or around your eyes, and low sodium levels which can cause weakness, feeling unsteady, confusion, problems concentrating, thinking or memory problems, bruising easily, frequent nosebleeds, frequent bleeding from your gums while brushing your teeth or flossing, dark, tar-like stool, bleeding from wounds that's hard to stop, lung disease or pneumonia. These last two can cause shortness of breath that gets worse, cough, or chest discomfort (See [11] for statistics on side effect occurance rates).
Taking venlafaxine with certain medications raises your risk of side effects. Examples of these drugs include:
Cimetidine
Taking this drug with venlafaxine raises your risk of high blood pressure or liver disease. These risks are greater if you are a senior.
Haloperidol
Taking this drug with venlafaxine raises your risk of QT prolongation. This is a heart condition with symptoms such as dizziness and an irregular heart rhythm.
Warfarin
Taking this drug with venlafaxine raises your risk of bleeding. Your doctor will monitor you closely, especially when starting or stopping your venlafaxine therapy. Tell your doctor right away if you notice any abnormal bleeding or bruising.
Anti-inflammatory drugs such as aspirin, ibuprofen, naproxen, and ketoprofen
Taking any of these drugs with venlafaxine raises your risk of bleeding. Your doctor will monitor you closely, especially when starting or stopping your venlafaxine therapy. Tell your doctor right away if you notice any abnormal bleeding or bruising.
Drugs such as ritonavir, clarithromycin, or ketoconazole
Drugs such as ritonavir, clarithromycin, or ketoconazole can slow the breakdown of drugs in your body. If you take any of these drugs with venlafaxine, the amount of venlafaxine may build up in your body. This would increase your risk of side effects.
Drugs that cause drowsiness, such as zolpidem, lorazepam, and diphenhydramine
Taking any of these drugs with venlafaxine may make the sleepiness from venlafaxine even worse.
Other drugs that can increase serotonin levels, such as fluoxetine, paroxetine, citalopram, duloxetine, linezolid, lithium, tramadol, and methylene blue
Venlafaxine increases your levels of serotonin. Taking it with any of these drugs may increase your serotonin levels even more. If your serotonin levels are too high, a life-threatening condition called serotonin syndrome can occur. Your doctor will monitor you closely when starting or increasing your dosage of either drug.
Certain drugs for migraine, called triptans, such as sumatriptan, rizatriptan, and zolmitriptan
Venlafaxine increases your levels of serotonin. Taking it with any of these drugs may increase your serotonin levels even more. If your serotonin levels are too high, a life-threatening condition called serotonin syndrome can occur. Your doctor will monitor you closely when starting or increasing your dosage of either drug.
Metoprolol
Metoprolol may be less effective when you take it with venlafaxine. This may cause your blood pressure to rise. Talk to your doctor before taking these drugs together.
Warnings
Venlafaxine has a “black box warning” which is the most dangerous the FDA can allow. This is because it can cause suicidal tendencies or thoughts during the first few weeks of trying it or during dose changes. This can also interfere with drug testing or increase your blood pressure.
DO NOT DRINK ALCOHOL TAKE MAOI’s OR WEIGHTLOSS PILLS WHILE TAKING VENLAFAXINE.
People with liver disease
If you have a history of liver disease, your liver may not process this drug as quickly as it should. This could lead to a buildup of this drug in your body. Your doctor may start you on a reduced dosage. If they increase your dosage later, they will monitor you closely.
People with kidney disease
If you have kidney disease or a history of kidney disease, you may not be able to clear this drug from your body well. This may increase the levels of venlafaxine in your body. This can cause more side effects. Your doctor may start you on a low dosage and monitor you closely if they increase your dosage.
People with heart problems
Venlafaxine can increase your heart rate, especially if you’re taking doses greater than 200 mg per day. If you have heart failure or if you’ve recently had a heart attack, your heart may not be able to tolerate this side effect.
People with hyperthyroidism
Hyperthyroidism can increase your heart rate. Venlafaxine can also increase your heart rate. If you have hyperthyroidism and take venlafaxine, your heart rate may increase to a dangerous level. You are especially at risk if you take venlafaxine doses greater than 200 mg per day.
People with a history of seizures
Venlafaxine raises your risk of seizures. If you have a seizure, stop taking venlafaxine and call your doctor right away.
People with increased eye pressure (glaucoma)
Venlafaxine can widen your pupils and block the flow of fluid in your eye. These effects can increase the pressure in your eyes. People with a history of increased eye pressure or glaucoma should have their eye pressure checked regularly while taking venlafaxine. Do not take venlafaxine if you have uncontrolled angle-closure glaucoma.
Pregnant women
Venlafaxine is a category C pregnancy drug. That means two things:
1.) Research in animals has shown adverse effects to the fetus when the mother takes the drug or
2.) There haven’t been enough studies done in humans to be certain how the drug might affect the fetus.
Talk to your doctor if you’re pregnant or plan to become pregnant. This drug should only be used if the potential benefit justifies the potential risk to the fetus.
Women who are breastfeeding
Venlafaxine may pass into breast milk and cause side effects in a child who is breastfed. Talk to your doctor about breastfeeding your child. You may need to decide whether to stop breastfeeding or stop taking this medication.
For seniors
The kidneys of older adults may not work as well as they used to. This can cause your body to process drugs more slowly. As a result, more of a drug stays in your body for a longer time. This raises your risk of side effects. Older adults may be at higher risk than younger people for low sodium levels in their blood when taking venlafaxine.
For children
This drug should not be used in people younger than 18 years of age.
When to call the doctor
Call your doctor right away if you become pregnant while taking this drug.
Also call your doctor if you don’t think your depression is getting better while you’re taking venlafaxine. It may take more than several months of antidepressant therapy to treat an episode of depression. If you don’t think your depression or anxiety is getting better, do not stop taking venlafaxine without talking to your doctor first. Your doctor will need to decrease your dosage over time to avoid serious symptoms from stopping venlafaxine too quickly.
Allergies
Venlafaxine can cause a severe allergic reaction. Symptoms can include trouble breathing, swelling of your face, tongue, eyes, or mouth, rash, hives, or blisters, alone or with joint paint or fever. If you have an allergic reaction, call your doctor or local poison control center right away. If your symptoms are severe, call 9-1-1 or go to the nearest emergency room. Don’t take this drug again if you’ve ever had an allergic reaction to it. Taking it again could be fatal.
Venlafaxine comes with serious risks if you don’t take it as prescribed, stop taking the drug suddenly or don’t take it at all.
Your depression or anxiety may not get better and may get worse. Do not stop venlafaxine without talking to your doctor. Stopping venlafaxine too quickly can cause serious symptoms such as anxiety, irritability, tiredness, restlessness, trouble sleeping, headache, sweating, dizziness, tingling or “pins and needles” feeling, shaking, confusion, nightmares, nausea, vomiting, or diarrhea. If this happens, your doctor may have you start taking venlafaxine again and decrease your dosage slowly.
If you take too much you could have dangerous levels of the drug in your body. This can lead to death. Symptoms of an overdose of this drug can include fast heart rate, unusual sleepiness, enlarged pupils, seizure, vomiting, heart rhythm changes, low blood pressure, muscle aches or pains, and dizziness. If you think you’ve taken too much of this drug, call your doctor or local poison control center. If your symptoms are severe, call 9-1-1 or go to the nearest emergency room right away.
If you miss doses or don’t take the drug on schedule your medication may not work as well or may stop working completely. For this drug to work well, a certain amount needs to be in your body at all times.
What to do if you miss a dose
Take your dose as soon as you remember. If you remember just a few hours before your next scheduled dose, take only one dose. Never try to catch up by taking two doses at once. This could result in dangerous side effects.
How to tell if the drug is working-The symptoms of your depression or anxiety should be less severe or happen less often.
Venlafaxine is used for long-term treatment. See [2] for full information
Venlafaxine has a “black box warning” which is the most dangerous the FDA can allow. This is because it can cause suicidal tendencies or thoughts during the first few weeks of trying it or during dose changes. This can also interfere with drug testing or increase your blood pressure.
DO NOT DRINK ALCOHOL TAKE MAOI’s OR WEIGHTLOSS PILLS WHILE TAKING VENLAFAXINE.
People with liver disease
If you have a history of liver disease, your liver may not process this drug as quickly as it should. This could lead to a buildup of this drug in your body. Your doctor may start you on a reduced dosage. If they increase your dosage later, they will monitor you closely.
People with kidney disease
If you have kidney disease or a history of kidney disease, you may not be able to clear this drug from your body well. This may increase the levels of venlafaxine in your body. This can cause more side effects. Your doctor may start you on a low dosage and monitor you closely if they increase your dosage.
People with heart problems
Venlafaxine can increase your heart rate, especially if you’re taking doses greater than 200 mg per day. If you have heart failure or if you’ve recently had a heart attack, your heart may not be able to tolerate this side effect.
People with hyperthyroidism
Hyperthyroidism can increase your heart rate. Venlafaxine can also increase your heart rate. If you have hyperthyroidism and take venlafaxine, your heart rate may increase to a dangerous level. You are especially at risk if you take venlafaxine doses greater than 200 mg per day.
People with a history of seizures
Venlafaxine raises your risk of seizures. If you have a seizure, stop taking venlafaxine and call your doctor right away.
People with increased eye pressure (glaucoma)
Venlafaxine can widen your pupils and block the flow of fluid in your eye. These effects can increase the pressure in your eyes. People with a history of increased eye pressure or glaucoma should have their eye pressure checked regularly while taking venlafaxine. Do not take venlafaxine if you have uncontrolled angle-closure glaucoma.
Pregnant women
Venlafaxine is a category C pregnancy drug. That means two things:
1.) Research in animals has shown adverse effects to the fetus when the mother takes the drug or
2.) There haven’t been enough studies done in humans to be certain how the drug might affect the fetus.
Talk to your doctor if you’re pregnant or plan to become pregnant. This drug should only be used if the potential benefit justifies the potential risk to the fetus.
Women who are breastfeeding
Venlafaxine may pass into breast milk and cause side effects in a child who is breastfed. Talk to your doctor about breastfeeding your child. You may need to decide whether to stop breastfeeding or stop taking this medication.
For seniors
The kidneys of older adults may not work as well as they used to. This can cause your body to process drugs more slowly. As a result, more of a drug stays in your body for a longer time. This raises your risk of side effects. Older adults may be at higher risk than younger people for low sodium levels in their blood when taking venlafaxine.
For children
This drug should not be used in people younger than 18 years of age.
When to call the doctor
Call your doctor right away if you become pregnant while taking this drug.
Also call your doctor if you don’t think your depression is getting better while you’re taking venlafaxine. It may take more than several months of antidepressant therapy to treat an episode of depression. If you don’t think your depression or anxiety is getting better, do not stop taking venlafaxine without talking to your doctor first. Your doctor will need to decrease your dosage over time to avoid serious symptoms from stopping venlafaxine too quickly.
Allergies
Venlafaxine can cause a severe allergic reaction. Symptoms can include trouble breathing, swelling of your face, tongue, eyes, or mouth, rash, hives, or blisters, alone or with joint paint or fever. If you have an allergic reaction, call your doctor or local poison control center right away. If your symptoms are severe, call 9-1-1 or go to the nearest emergency room. Don’t take this drug again if you’ve ever had an allergic reaction to it. Taking it again could be fatal.
Venlafaxine comes with serious risks if you don’t take it as prescribed, stop taking the drug suddenly or don’t take it at all.
Your depression or anxiety may not get better and may get worse. Do not stop venlafaxine without talking to your doctor. Stopping venlafaxine too quickly can cause serious symptoms such as anxiety, irritability, tiredness, restlessness, trouble sleeping, headache, sweating, dizziness, tingling or “pins and needles” feeling, shaking, confusion, nightmares, nausea, vomiting, or diarrhea. If this happens, your doctor may have you start taking venlafaxine again and decrease your dosage slowly.
If you take too much you could have dangerous levels of the drug in your body. This can lead to death. Symptoms of an overdose of this drug can include fast heart rate, unusual sleepiness, enlarged pupils, seizure, vomiting, heart rhythm changes, low blood pressure, muscle aches or pains, and dizziness. If you think you’ve taken too much of this drug, call your doctor or local poison control center. If your symptoms are severe, call 9-1-1 or go to the nearest emergency room right away.
If you miss doses or don’t take the drug on schedule your medication may not work as well or may stop working completely. For this drug to work well, a certain amount needs to be in your body at all times.
What to do if you miss a dose
Take your dose as soon as you remember. If you remember just a few hours before your next scheduled dose, take only one dose. Never try to catch up by taking two doses at once. This could result in dangerous side effects.
How to tell if the drug is working-The symptoms of your depression or anxiety should be less severe or happen less often.
Venlafaxine is used for long-term treatment. See [2] for full information
References
[1] "Venlafaxine (Effexor)." Venlafaxine (Effexor) - EMedExpert.com. EMedExpert.com, 31 Mar. 2008. Web. 04 Dec. 2016.<http://www.emedexpert.com/facts/venlafaxine-facts.shtml>
[2] "Venlafaxine, Oral Tablet." Venlafaxine | Side Effects, Dosage, Uses & More. University of Illinois-Chicago, Drug Information Group, 16 Mar. 2016. Web. 04 Dec. 2016. <http://www.healthline.com/drugs/venlafaxine/oral-tablet#Highlights1>.
[3] Guzman, Favio, MD. "Venlafaxine and Desvenlafaxine: Differences and Similarities." Psychopharmacology Institute. N.p., n.d. Web. 04 Dec. 2016. <http://psychopharmacologyinstitute.com/antidepressants/snris/venlafaxine-desvenlafaxine-differences-similarities/>.
[4] Laura Enzor. "What Is Norepinephrine? - Effects, Function & Definition." Study.com. N.p., n.d. Web. 04 Dec. 2016. <http://study.com/academy/lesson/what-is-norepinephrine-effects-function-definition.html>.
[5] Hood, S. D., 1st, J. K. Melichar, L. G. Taylor, N. Kalk, T. R. Edwards, D. A. Hince, A. Lenox-Smith, A. R. Lingford-Hughes, and D. J. Nutt. "Noradrenergic Function in Generalized Anxiety Disorder: Impact of Treatment with Venlafaxine on the Physiological and Psychological Responses to Clonidine Challenge." Journal of Psychopharmacology (Oxford, England). U.S. National Library of Medicine, 21 Jan. 2010. Web. 04 Dec. 2016. <https://www.ncbi.nlm.nih.gov/pubmed/20093317>.
[6] Fink, Jennifer. "Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)." Healthline. N.p., 10 Dec. 2013. Web. 04 Dec. 2016. <http://www.healthline.com/health/depression/serotonin-norepinephrine-reuptake-inhibitors-snris>.
[7] Piascik, M. T. "ADRENERGIC PHARMACOLOGY." ADRENERGIC PHARMACOLOGY. N.p., n.d. Web. 04 Dec. 2016. <http://www.uky.edu/~mtp/OBI836AR.html>.
[8] Sargis, Robert M., MD, PhD. "An Overview of the Adrenal Glands." EndocrineWeb. N.p., 8 Apr. 2015. Web. 04 Dec. 2016. <http://www.endocrineweb.com/endocrinology/overview-adrenal-glands>.
[9] Bennington, Vanessa. "Understanding Our Adrenal System: Norepinephrine." Breaking Muscle. N.p., n.d. Web. 04 Dec. 2016. <https://breakingmuscle.com/learn/understanding-our-adrenal-system-norepinephrine>.
[10] "Definition of Catecholamine." MedicineNet. N.p., 13 Mar. 2016. Web. 04 Dec. 2016. <http://www.medicinenet.com/script/main/art.asp?articlekey=20210>.
[11] Square, Albert. New York: Garland, 1974. Norepenephrine. Web. 4 Dec. 2016. <http://www.caam.rice.edu/~cox/wrap/norepinephrine.pdf>.
[12] Mayo Clinic Staff. "Depression (major Depressive Disorder)." Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs) - Mayo Clinic. Mayo Clinic, 21 June 2016. Web. 04 Dec. 2016. <http://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20044970>.
[1] "Venlafaxine (Effexor)." Venlafaxine (Effexor) - EMedExpert.com. EMedExpert.com, 31 Mar. 2008. Web. 04 Dec. 2016.<http://www.emedexpert.com/facts/venlafaxine-facts.shtml>
[2] "Venlafaxine, Oral Tablet." Venlafaxine | Side Effects, Dosage, Uses & More. University of Illinois-Chicago, Drug Information Group, 16 Mar. 2016. Web. 04 Dec. 2016. <http://www.healthline.com/drugs/venlafaxine/oral-tablet#Highlights1>.
[3] Guzman, Favio, MD. "Venlafaxine and Desvenlafaxine: Differences and Similarities." Psychopharmacology Institute. N.p., n.d. Web. 04 Dec. 2016. <http://psychopharmacologyinstitute.com/antidepressants/snris/venlafaxine-desvenlafaxine-differences-similarities/>.
[4] Laura Enzor. "What Is Norepinephrine? - Effects, Function & Definition." Study.com. N.p., n.d. Web. 04 Dec. 2016. <http://study.com/academy/lesson/what-is-norepinephrine-effects-function-definition.html>.
[5] Hood, S. D., 1st, J. K. Melichar, L. G. Taylor, N. Kalk, T. R. Edwards, D. A. Hince, A. Lenox-Smith, A. R. Lingford-Hughes, and D. J. Nutt. "Noradrenergic Function in Generalized Anxiety Disorder: Impact of Treatment with Venlafaxine on the Physiological and Psychological Responses to Clonidine Challenge." Journal of Psychopharmacology (Oxford, England). U.S. National Library of Medicine, 21 Jan. 2010. Web. 04 Dec. 2016. <https://www.ncbi.nlm.nih.gov/pubmed/20093317>.
[6] Fink, Jennifer. "Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs)." Healthline. N.p., 10 Dec. 2013. Web. 04 Dec. 2016. <http://www.healthline.com/health/depression/serotonin-norepinephrine-reuptake-inhibitors-snris>.
[7] Piascik, M. T. "ADRENERGIC PHARMACOLOGY." ADRENERGIC PHARMACOLOGY. N.p., n.d. Web. 04 Dec. 2016. <http://www.uky.edu/~mtp/OBI836AR.html>.
[8] Sargis, Robert M., MD, PhD. "An Overview of the Adrenal Glands." EndocrineWeb. N.p., 8 Apr. 2015. Web. 04 Dec. 2016. <http://www.endocrineweb.com/endocrinology/overview-adrenal-glands>.
[9] Bennington, Vanessa. "Understanding Our Adrenal System: Norepinephrine." Breaking Muscle. N.p., n.d. Web. 04 Dec. 2016. <https://breakingmuscle.com/learn/understanding-our-adrenal-system-norepinephrine>.
[10] "Definition of Catecholamine." MedicineNet. N.p., 13 Mar. 2016. Web. 04 Dec. 2016. <http://www.medicinenet.com/script/main/art.asp?articlekey=20210>.
[11] Square, Albert. New York: Garland, 1974. Norepenephrine. Web. 4 Dec. 2016. <http://www.caam.rice.edu/~cox/wrap/norepinephrine.pdf>.
[12] Mayo Clinic Staff. "Depression (major Depressive Disorder)." Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs) - Mayo Clinic. Mayo Clinic, 21 June 2016. Web. 04 Dec. 2016. <http://www.mayoclinic.org/diseases-conditions/depression/in-depth/antidepressants/art-20044970>.
